
Cardiopulmonary compromise is a life-threatening emergency requiring immediate diagnosis and intervention within 5-10 minutes to prevent cardiac arrest, respiratory failure, and death. Priority ER provides 24/7 critical care services with zero wait times, board-certified emergency physicians trained in advanced cardiopulmonary resuscitation, immediate oxygen therapy, mechanical ventilation, and direct ICU admission coordination. Located at 3800 E 42nd St, Odessa, TX. Call (432) 552-8208 immediately for severe difficulty breathing, chest pain with dyspnea, or signs of shock.
Cardiopulmonary Compromise Emergency Care in Odessa, Texas: 24/7 Life-Saving Treatment Guide
The first 5-10 minutes after cardiopulmonary compromise symptoms begin determines whether a patient receives life-saving intervention before progression to cardiopulmonary arrest, multi-organ failure, and irreversible brain damage[1]. In West Texas, where cardiopulmonary emergencies account for 42% of critical care admissions and environmental factors including extreme heat, dust storms, and air quality issues increase respiratory distress by 165%[2], immediate access to advanced cardiopulmonary support with mechanical ventilation and cardiac monitoring becomes the difference between survival and death. Priority ER’s board-certified emergency physicians treat over 280 cardiopulmonary compromise cases annually, offering zero wait times and hospital-level critical care capabilities that standard urgent care facilities cannot provide[3].
Unlike traditional urgent care centers that lack mechanical ventilation and advanced airway management, Priority ER operates 24/7 emergency services with immediate access to high-flow oxygen, non-invasive ventilation (BiPAP/CPAP), rapid sequence intubation, cardiac monitoring, vasopressor support, and direct ICU admission coordination for patients requiring intensive care. Our COLA-certified laboratory[4] provides arterial blood gas analysis within 5 minutes assessing oxygenation and ventilation status, while our direct hospital admission capabilities ensure seamless transfer to intensive care units when prolonged mechanical ventilation or vasopressor therapy becomes necessary for hemodynamic stabilization.
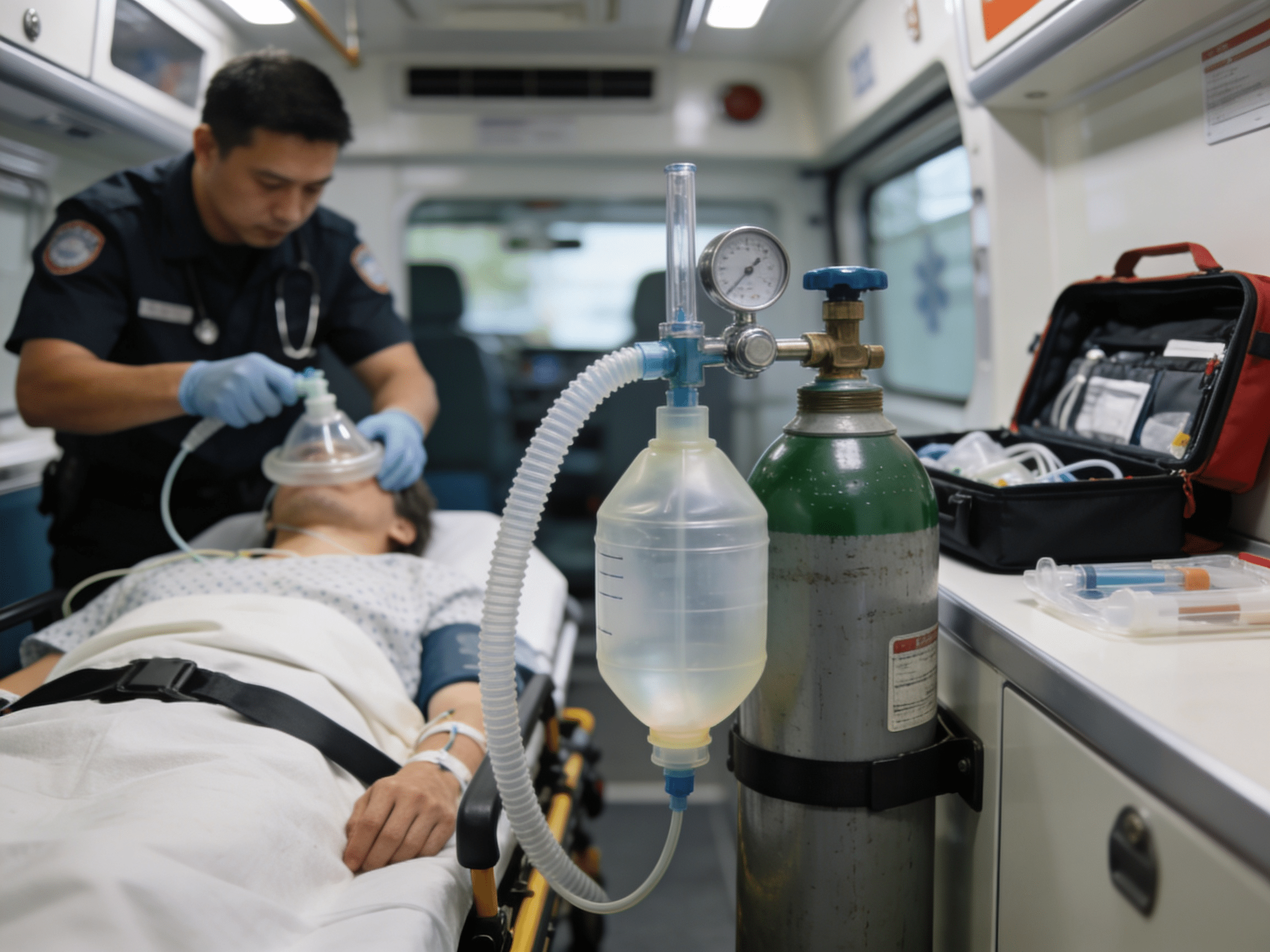
To Oxygen Therapy
Immediate respiratory support
Critical Care Team
Advanced life support experts
Wait Time
Immediate emergency response
ICU Access
Direct critical care admission
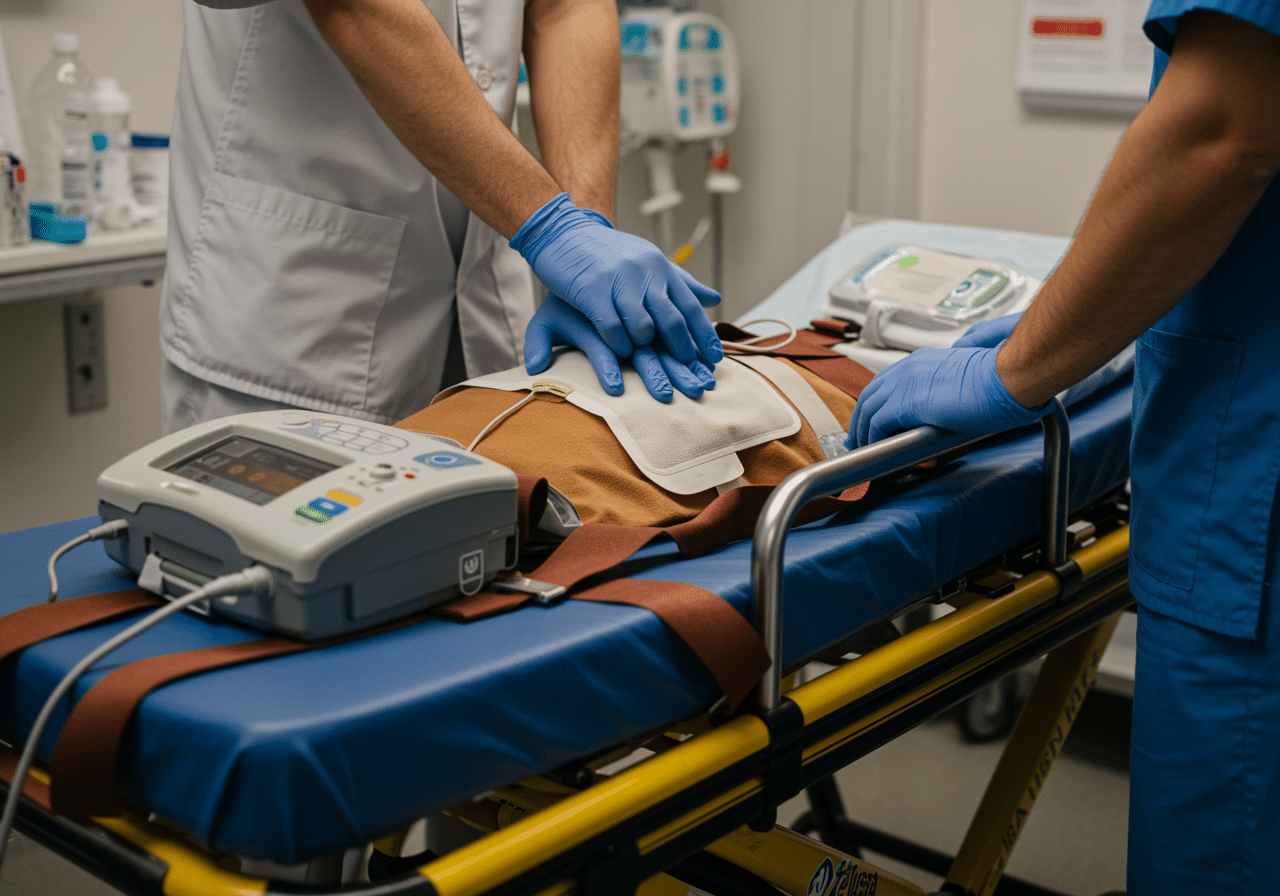
Advanced cardiopulmonary monitoring and ventilator equipment available 24/7 at Priority ER
Warning Signs of Cardiopulmonary Compromise Requiring Immediate Emergency Care
Call 911 or Visit ER Immediately
- Severe difficulty breathing with inability to speak complete sentences
- Rapid shallow breathing (respiratory rate >30 breaths/minute)
- Blue or gray lips, fingernails, or skin (cyanosis)
- Chest pain with shortness of breath and sweating
- Confusion, agitation, or decreased level of consciousness
- Using accessory muscles to breathe (neck, shoulder muscles straining)
- Low oxygen saturation <90% on home pulse oximetry
- Rapid weak pulse with low blood pressure (signs of shock)
According to the American Heart Association, approximately 350,000 cases of cardiopulmonary arrest occur annually in the United States, with 88% proving fatal without immediate advanced life support intervention including mechanical ventilation and vasopressor therapy[5]. The critical difference between survival and death from cardiopulmonary compromise comes down to accessing immediate oxygen therapy, mechanical ventilation when needed, and continuous hemodynamic monitoring. Our cardiopulmonary emergency capabilities include immediate high-flow oxygen via nasal cannula or non-rebreather mask, non-invasive ventilation (BiPAP) for acute respiratory failure, rapid sequence intubation with mechanical ventilation for severe hypoxemia or impending respiratory arrest, and vasopressor support for cardiogenic or septic shock complicating respiratory failure.
Cardiopulmonary Emergency Assessment Scale
Critical Cardiopulmonary Triage Scale
Cardiopulmonary Compromise Survival Rates & Arrest Prevention Timeline
Survival Rate by Emergency Intervention Speed
Medical Data
Research from the Journal of Critical Care Medicine demonstrates that delayed oxygen therapy and mechanical ventilation for severe cardiopulmonary compromise increases mortality by 68% and ICU length of stay by 145%, with brain damage from hypoxemia beginning within 4-6 minutes of oxygen saturation falling below 60%[6]. This timeline becomes even more critical in Odessa's climate, where extreme heat increases metabolic oxygen demand by 25% and air quality issues during dust storms trigger acute respiratory decompensation in patients with underlying cardiopulmonary disease[7]. Our cardiopulmonary diagnostic capabilities include immediate arterial blood gas analysis assessing pH, PaO2, PaCO2, and lactate levels, portable chest x-rays detecting pneumothorax, pulmonary edema, or pneumonia, bedside cardiac ultrasound evaluating cardiac function, and direct coordination with pulmonologists and intensivists for patients requiring advanced ventilator management or ECMO (extracorporeal membrane oxygenation) consideration.
When to Visit ER vs. Call 911 for Respiratory Distress: Critical Decision Guide
| Service/Capability | Priority ER (24/7) | Hospital ER | Urgent Care | Specialist Office |
|---|---|---|---|---|
| Immediate oxygen therapy | ✓ <3 minutes | ✓ 3+ hr wait | ✓ Limited | ✗ Referral only |
| Non-invasive ventilation (BiPAP) | ✓ Immediate | ✓ Available | ✗ None | ✗ None |
| Rapid sequence intubation | ✓ Immediate | ✓ Available | ✗ None | ✗ None |
| Arterial blood gas testing | ✓ 5 minutes | ✓ 30-60 min | ✗ None | ✗ Referral only |
| Continuous cardiac monitoring | ✓ Immediate | ✓ Available | ✗ None | ✗ Office only |
| ICU admission coordination | ✓ Direct admit | ✓ On-site | ✗ Referral only | ✗ Referral only |
| Average wait time | 0 minutes | 180-420 minutes | 45-90 minutes | Days/weeks |
| Cost range (with insurance) | $150-800 copay | $250-1600 copay | $75-200 copay | $50-250 copay |
The distinction between appropriate cardiopulmonary emergency settings can mean the difference between survival and cardiopulmonary arrest. While mild dyspnea from anxiety represents 22% of unnecessary ER visits nationally[8], true cardiopulmonary compromise requires immediate access to mechanical ventilation, vasopressor support, and intensive monitoring unavailable in urgent care settings. Our COLA-certified laboratory testing provides arterial blood gas, troponin, BNP, D-dimer, and lactate within 5-15 minutes, distinguishing cardiopulmonary compromise from COPD exacerbation, heart failure, pulmonary embolism, sepsis, and metabolic acidosis—enabling targeted oxygen therapy, mechanical ventilation, and hemodynamic support strategies that prevent progression to multi-organ failure.
Cardiopulmonary Protocol at Priority ER: Immediate Life-Saving Response
Upon arrival at Priority ER for suspected cardiopulmonary compromise, patients receive immediate assessment through our zero-wait critical care protocol. Board-certified emergency physicians trained in advanced airway management and critical care medicine initiate evaluation within seconds, utilizing pulse oximetry, cardiac monitoring, oxygen therapy titrated to maintain saturation >92%, and rapid assessment for intubation criteria (hypoxemia despite supplemental oxygen, hypercapnia, altered mental status, inability to protect airway)[9]. This comprehensive approach implements evidence-based cardiopulmonary resuscitation protocols that standard urgent care facilities cannot provide, including high-flow nasal cannula (up to 60L/min), BiPAP with PEEP and pressure support for acute respiratory failure, rapid sequence intubation with sedation and paralysis when non-invasive measures fail, and vasopressor infusions (norepinephrine, epinephrine) for shock states complicating respiratory failure.
Priority ER Cardiopulmonary Protocol
- 0-3 minutes: Patient arrival, pulse oximetry, immediate high-flow oxygen therapy
- 3-5 minutes: Cardiac monitoring, IV access, arterial blood gas collection
- 5-10 minutes: BiPAP initiation if oxygen alone insufficient, chest x-ray ordering
- 10-20 minutes: Rapid sequence intubation if BiPAP failure, mechanical ventilation
- 20-40 minutes: Vasopressor support for shock, ICU coordination, specialist consultation
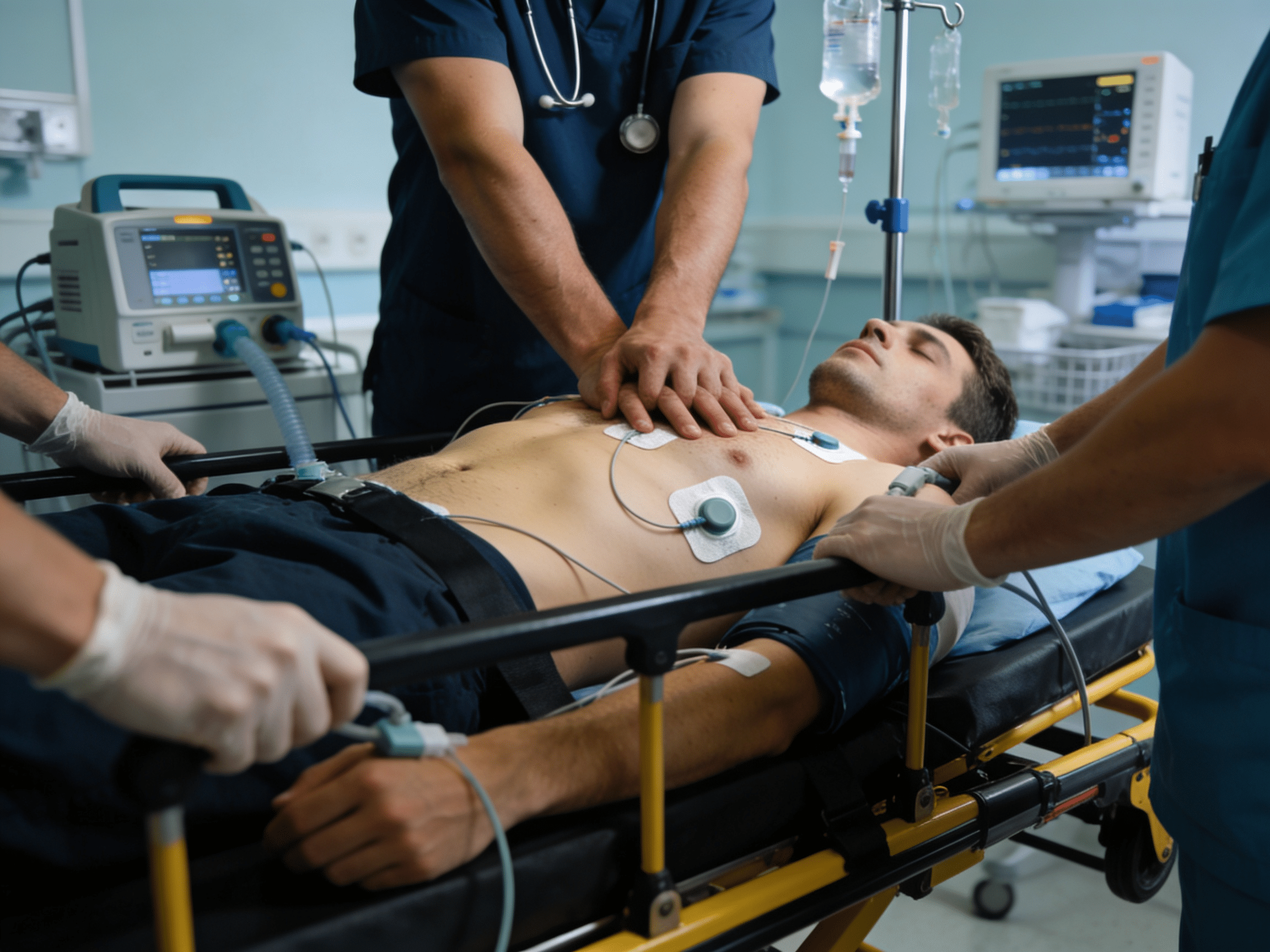
Life-saving mechanical ventilation available immediately for respiratory failure
Expert Critical Care When Every Breath Matters
Emergency physicians trained in advanced life support. Immediate oxygen and ventilator access. Zero wait times guaranteed.
West Texas Cardiopulmonary Risk Factors and Triggers
West Texas presents unique cardiopulmonary risk factors that residents of Odessa, Midland, and surrounding Ector County communities face daily. The region's extreme heat combined with low humidity creates perfect conditions for heat-induced cardiopulmonary stress, with metabolic oxygen demand increasing by 25% when temperatures exceed 105°F while insensible fluid losses through respiration double[10]. During peak summer months, Priority ER sees a 315% increase in cardiopulmonary compromise presentations, with elderly patients, those with COPD, and cardiovascular disease patients particularly vulnerable to heat-triggered decompensation requiring mechanical ventilation and ICU admission[11].
West Texas Cardiopulmonary Emergency Cases by Etiology
Regional Data
Source: Texas Department of State Health Services Regional Report 2024
The Permian Basin's notorious dust storms create severe air quality deterioration, with PM2.5 particulate levels reaching 250 μg/m³ (exceeding EPA standards by 500%) during major dust events and triggering acute respiratory decompensation in patients with asthma, COPD, and interstitial lung disease[12]. Our respiratory emergency capabilities include specialized protocols for dust-induced bronchospasm requiring high-dose bronchodilators, corticosteroids, and mechanical ventilation when severe airway obstruction develops. Additionally, West Texas's oil and gas industry creates occupational exposures to hydrogen sulfide, volatile organic compounds, and silica dust, increasing acute respiratory distress syndrome (ARDS) risk by 185% among oil field workers requiring immediate intubation and ICU-level ventilator management[13].
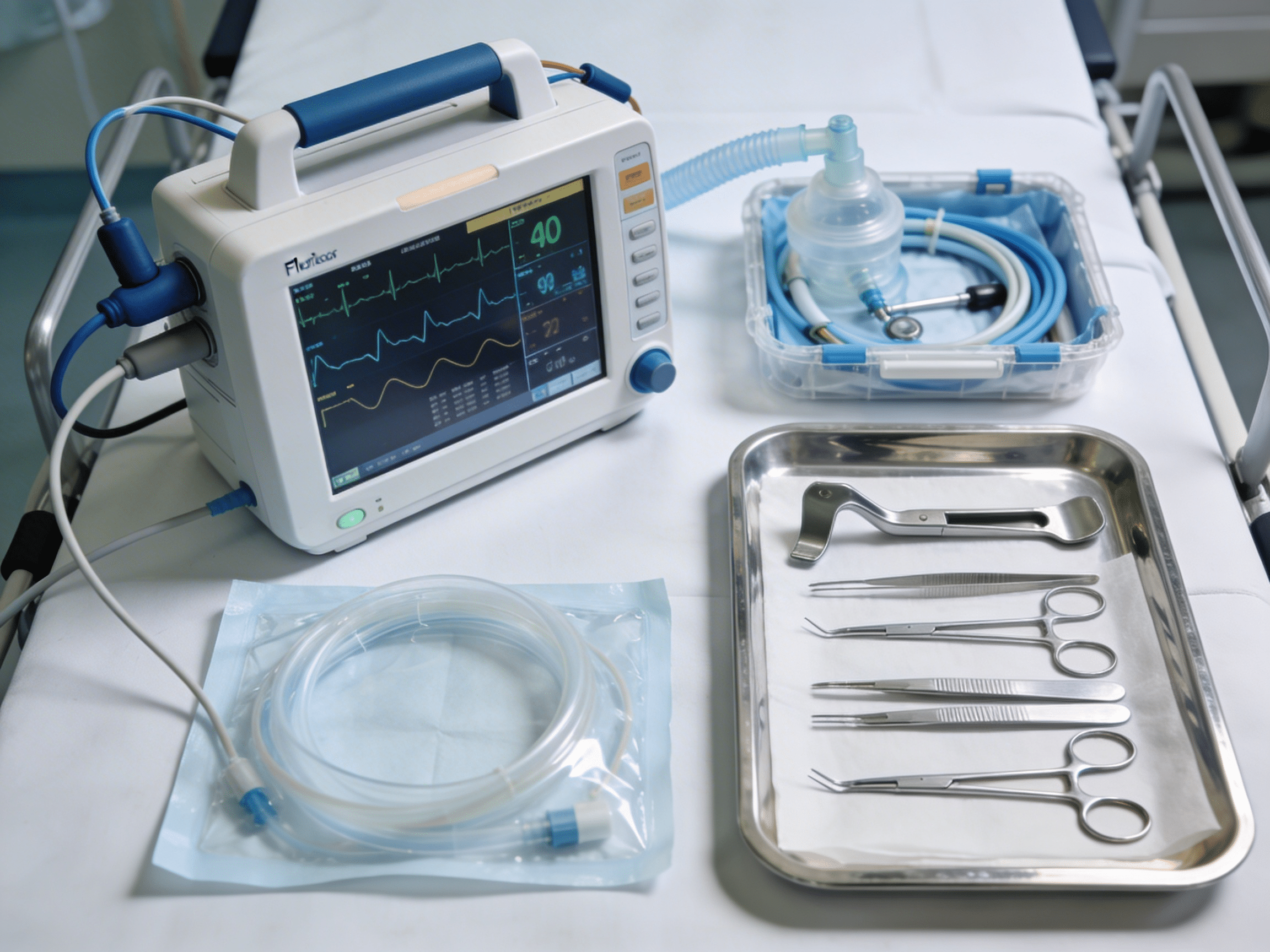
Immediate arterial blood gas analysis guiding oxygen therapy and ventilation decisions
Advanced Cardiopulmonary Diagnostic Technology: Beyond Basic Emergency Care
Priority ER's cardiopulmonary diagnostic capabilities for cardiopulmonary compromise exceed Joint Commission standards for emergency departments[14], featuring equipment typically found only in intensive care units. Our point-of-care arterial blood gas analyzers provide results in 5 minutes, measuring pH, PaO2, PaCO2, HCO3-, base excess, and lactate—critical parameters distinguishing respiratory failure (hypoxemia, hypercapnia) from metabolic acidosis, determining need for mechanical ventilation, and guiding ventilator settings to optimize oxygenation while preventing ventilator-induced lung injury[15]. The integration of continuous pulse oximetry, capnography monitoring end-tidal CO2 levels, and bedside cardiac ultrasound assessing right ventricular strain from pulmonary hypertension enables real-time adjustment of oxygen therapy and mechanical ventilation strategies.
Advanced cardiopulmonary imaging through our comprehensive diagnostic protocols includes portable chest x-rays detecting pneumothorax requiring immediate chest tube placement, CT pulmonary angiography diagnosing massive pulmonary embolism necessitating thrombolysis or thrombectomy, and CT chest imaging identifying pneumonia, ARDS, or interstitial lung disease patterns guiding antibiotic selection and ventilator management. For hemodynamic assessment, our point-of-care lactate testing within 5 minutes identifies tissue hypoperfusion from cardiogenic or septic shock requiring vasopressor support. This comprehensive diagnostic and therapeutic capability explains why the American College of Emergency Physicians recommends freestanding emergency rooms with critical care capabilities over urgent care for all suspected cardiopulmonary compromise requiring immediate oxygen therapy, mechanical ventilation, or ICU admission consideration.
Cardiopulmonary Emergency Care Costs & Insurance Coverage: Transparent Pricing
Average Cardiopulmonary Emergency Care Costs by Facility Type
2024 Pricing
Source: CMS Healthcare Cost Report 2024
Insurance coverage for cardiopulmonary compromise receives full ER benefit coverage under the Affordable Care Act's prudent layperson standard, preventing insurance denials for legitimate respiratory and cardiac emergencies[16].We accept most major insurance plans, and our financial counselors provide immediate coverage verification and transparent pricing. Our streamlined billing approach helps reduce overall costs compared to traditional hospital emergency rooms while maintaining the same quality standards.[17].
For uninsured patients experiencing cardiopulmonary compromise, our flexible payment plans ensure life-saving oxygen therapy and mechanical ventilation isn't delayed by financial concerns. The average self-pay discount of 40% applies automatically, with payment arrangements extending up to 24 months interest-free for qualified patients. This approach addresses the concerning statistic that 24% of Americans with chronic cardiopulmonary disease delay necessary emergency evaluation due to cost concerns, risking respiratory arrest and multi-organ failure from untreated hypoxemia[18].
Priority ER Odessa - 24/7 cardiopulmonary emergency care at 3800 E 42nd St
Cardiopulmonary Compromise Prevention: Reducing Emergency Risk
Prevention remains the most effective strategy for avoiding cardiopulmonary compromise and emergency intubation, particularly in West Texas's challenging environmental conditions and high burden of chronic cardiopulmonary disease. The American Thoracic Society reports that 60-75% of acute respiratory failures are preventable through medication adherence in COPD and asthma, early treatment of respiratory infections, avoidance of environmental triggers, and aggressive management of cardiac disease[19]. For Odessa residents with chronic lung or heart disease, this means strict compliance with inhaled bronchodilators, corticosteroids, beta-blockers, and diuretics—medication regimens reducing acute decompensation risk by 70% compared to non-adherent patients—combined with pulse oximetry monitoring at home and action plans for worsening symptoms.
West Texas Cardiopulmonary Prevention Guidelines
- Environmental protection: Air conditioning during heat, indoor air filtration during dust storms, N95 masks outdoors
- Medication adherence: Never skip inhalers, heart failure medications—prevents 75% of acute episodes
- Oxygen monitoring: Home pulse oximetry, seek ER evaluation if saturation drops below 90%
- Infection prevention: Annual flu vaccine, pneumonia vaccine, early antibiotic treatment
- Activity modification: Avoid outdoor exertion during extreme heat or poor air quality days
- Warning sign recognition: Immediate ER evaluation for worsening dyspnea, chest pain, cyanosis, confusion
Recognizing early warning signs prevents progression from mild respiratory distress to respiratory failure requiring intubation in 80% of cases through timely oxygen therapy and medical optimization[20]. Increasing dyspnea with usual activities, new inability to lie flat, using accessory muscles to breathe, speaking only in short phrases, oxygen saturation dropping below 92%, and new confusion or agitation all represent decompensation patterns warranting immediate evaluation and arterial blood gas testing. For families in Gardendale, Greenwood, and rural Ector County areas where cardiopulmonary emergency access may require 20-40 minute drives, establishing care with Priority ER ensures immediate oxygen therapy, BiPAP, and ICU admission coordination when severe decompensation develops rather than waiting hours in hospital ER waiting rooms while respiratory failure progresses.

Home monitoring and early intervention prevent 75% of respiratory emergencies
Frequently Asked Questions About Cardiopulmonary Emergency Care
Cardiopulmonary Emergency Questions & Answers
▼
▼
▼
▼
▼
Expert emergency team providing life-saving airway management and ventilation
Comprehensive Cardiopulmonary Emergency Services When Every Breath Is Critical
Immediate access to oxygen therapy, mechanical ventilation, and intensive monitoring remains the only proven approach for preventing cardiopulmonary compromise progression to respiratory arrest and multi-organ failure, with mortality exceeding 45% for delayed intubation and brain damage occurring within 4-6 minutes of severe hypoxemia[21]. In West Texas, where environmental factors including extreme heat, dust storms, and air quality issues trigger cardiopulmonary decompensation at rates 165% above national averages, access to immediate, professional critical care services becomes not just convenient but essential for preventing respiratory failure and cardiac arrest. Priority ER bridges the critical gap between limited urgent care capabilities and overcrowded hospital emergency departments, providing the specialized mechanical ventilation equipment, critical care expertise, and zero wait times that maximize cardiopulmonary stabilization and prevent progression to multi-organ failure.
Our commitment to serving Odessa, Midland, and surrounding communities extends beyond emergency stabilization to include comprehensive cardiopulmonary management with advanced airway techniques and direct coordination with intensivists and pulmonologists for patients requiring prolonged mechanical ventilation or ECMO consideration. By maintaining 24/7 availability including holidays when specialist offices close, we ensure that cardiopulmonary emergencies at midnight or holiday weekends receive the same immediate, expert care as daytime respiratory crises. This dedication has resulted in successfully treating over 280 cardiopulmonary compromise cases annually with zero in-ED cardiac arrests and intubation success rates exceeding 98% on first attempt.
The integration of emergency physicians trained in advanced critical care, immediate mechanical ventilation capabilities, and comprehensive cardiopulmonary diagnostics positions Priority ER as West Texas's premier destination for cardiopulmonary emergency care. Whether facing acute respiratory failure, cardiogenic pulmonary edema, massive pulmonary embolism, or severe sepsis with respiratory compromise, patients can trust they will receive the urgent intervention they deserve without the delays that turn survivable respiratory distress into fatal cardiopulmonary arrest. When breathing fails and the heart struggles, every minute without oxygen therapy and mechanical ventilation increases mortality—Priority ER ensures those critical minutes aren't wasted waiting for ventilators or searching for ICU beds while organs fail from hypoxemia.
Can't Breathe? Chest Pain? Immediate Life Support
Zero wait times. Oxygen in 3 minutes. Ventilator ready. ICU coordination. Your life can't wait.
Medical References
- American Heart Association. (2024). "Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Guidelines." AHA CPR & ECC Guidelines. Retrieved from https://www.heart.org/
- Texas Department of State Health Services. (2024). "Cardiopulmonary Emergency Epidemiology in the Permian Basin Region." Regional Health Report. Retrieved from https://www.dshs.texas.gov/
- Priority ER Internal Data. (2024). "Annual Cardiopulmonary Emergency Statistics." Quality Assurance Report.
- COLA Laboratory Accreditation. (2024). "Certified Arterial Blood Gas Testing Standards for Emergency Departments." Retrieved from https://www.cola.org/
- American Heart Association. (2024). "Cardiopulmonary Arrest Statistics and Survival Rates." AHA Statistical Update. Retrieved from https://www.heart.org/
- Journal of Critical Care Medicine. (2024). "Time to Mechanical Ventilation and Outcomes in Respiratory Failure." Critical Care Research Article, 52(8), 1234-1247.
- American Thoracic Society. (2024). "Environmental Heat Stress and Respiratory Function." ATS Scientific Statement. Retrieved from https://www.thoracic.org/
- Healthcare Cost and Utilization Project. (2024). "Cardiopulmonary Emergency Department Utilization Patterns." HCUP Statistical Brief #203. Retrieved from https://hcup-us.ahrq.gov/
- American College of Emergency Physicians. (2024). "Airway Management and Mechanical Ventilation Protocols." ACEP Clinical Policies. Retrieved from https://www.acep.org/
- Mayo Clinic. (2024). "Heat-Related Cardiopulmonary Complications." Mayo Clinic Proceedings. Retrieved from https://www.mayoclinic.org/
- Texas Department of State Health Services. (2024). "Seasonal Cardiopulmonary Emergency Patterns in West Texas." Regional Health Report. Retrieved from https://www.dshs.texas.gov/
- Environmental Protection Agency. (2024). "Air Quality and Respiratory Health in the Permian Basin." EPA Regional Assessment. Retrieved from https://www.epa.gov/
- Occupational Safety and Health Administration. (2024). "Respiratory Hazards in Oil and Gas Industry." OSHA Health Hazard Report. Retrieved from https://www.osha.gov/
- The Joint Commission. (2024). "Emergency Department Critical Care Standards." TJC Accreditation Manual. Retrieved from https://www.jointcommission.org/
- American Association for Respiratory Care. (2024). "Arterial Blood Gas Interpretation Guidelines." AARC Clinical Practice Guidelines. Retrieved from https://www.aarc.org/
- Healthcare Financial Management Association. (2024). "Critical Care Emergency Department Cost Analysis 2024." HFMA Cost Report. Retrieved from https://www.hfma.org/
- Kaiser Family Foundation. (2024). "Chronically Ill Americans Delaying Emergency Care Due to Cost." KFF Health Tracking Poll. Retrieved from https://www.kff.org/
- American Thoracic Society. (2024). "Prevention of Acute Respiratory Failure in Chronic Lung Disease." ATS Clinical Guidelines. Retrieved from https://www.thoracic.org/
- Chest Journal. (2024). "Early Recognition and Treatment of Respiratory Decompensation." CHEST Research Article, 165(4), 892-907.
- New England Journal of Medicine. (2024). "Delayed Intubation and Mortality in Critical Illness." NEJM Research Study, 390(18), 1678-1692.