
Pelvic ultrasound for ectopic pregnancy or ovarian torsion is a critical diagnostic test required immediately when experiencing severe pelvic pain with positive pregnancy test, sudden unilateral pain with nausea, vaginal bleeding with cramping, or dizziness suggesting internal bleeding. Priority ER provides 24/7 emergency pelvic ultrasound with zero wait times, board-certified emergency physicians interpreting results within 15 minutes, and OB/GYN consultation for ruptured ectopic requiring surgery or ovarian torsion requiring emergent detorsion. Located at 3800 E 42nd St, Odessa, TX. Call (432) 552-8208 immediately for emergency pelvic ultrasound evaluation.
Pelvic Ultrasound for Ectopic Pregnancy or Ovarian Torsion in Odessa, Texas: 24/7 Emergency Gynecological Imaging Guide
The first 60 minutes after ectopic pregnancy rupture can determine whether emergency surgery prevents hemorrhagic shock and death or delays cause exsanguination, with ruptured ectopic causing 6% of all maternal deaths in the first trimester[1]. In West Texas, where ectopic pregnancy affects 2% of all pregnancies and ovarian torsion occurs in 3% of women with ovarian masses, delayed ultrasound diagnosis increases ovarian necrosis rates by 285% when surgical intervention exceeds 8 hours[2], immediate access to pelvic ultrasound for ectopic pregnancy or ovarian torsion becomes critical for identifying life-threatening gynecological emergencies. Priority ER’s board-certified emergency physicians perform over 1,200 emergency pelvic ultrasound examinations annually, offering zero wait times and immediate OB/GYN consultation capabilities that standard urgent care facilities cannot provide[3].
Unlike traditional urgent care centers that lack ultrasound capabilities or close at 8 PM, Priority ER operates 24/7 emergency services with immediate access to transvaginal and transabdominal ultrasound, board-certified emergency physician-performed or interpreted imaging within 15 minutes, and direct OB/GYN consultation when ultrasound identifies ruptured ectopic requiring emergency laparoscopy, ovarian torsion requiring detorsion surgery, or hemorrhagic cyst requiring intervention. Our COLA-certified diagnostic imaging[4] ensures accurate detection of ectopic pregnancy (sensitivity 87-99% with β-hCG correlation), ovarian torsion (sensitivity 74-92% with Doppler assessment), and free fluid indicating rupture while our direct surgeon coordination ensures seamless care when imaging identifies gynecological emergencies requiring operative intervention within hours preventing hemorrhagic shock, ovarian loss, and death.
To Ultrasound
Immediate bedside imaging
Pelvic Ultrasound Available
Including holidays & weekends
Wait Time
Immediate evaluation
To OB/GYN Consult
Direct surgeon access
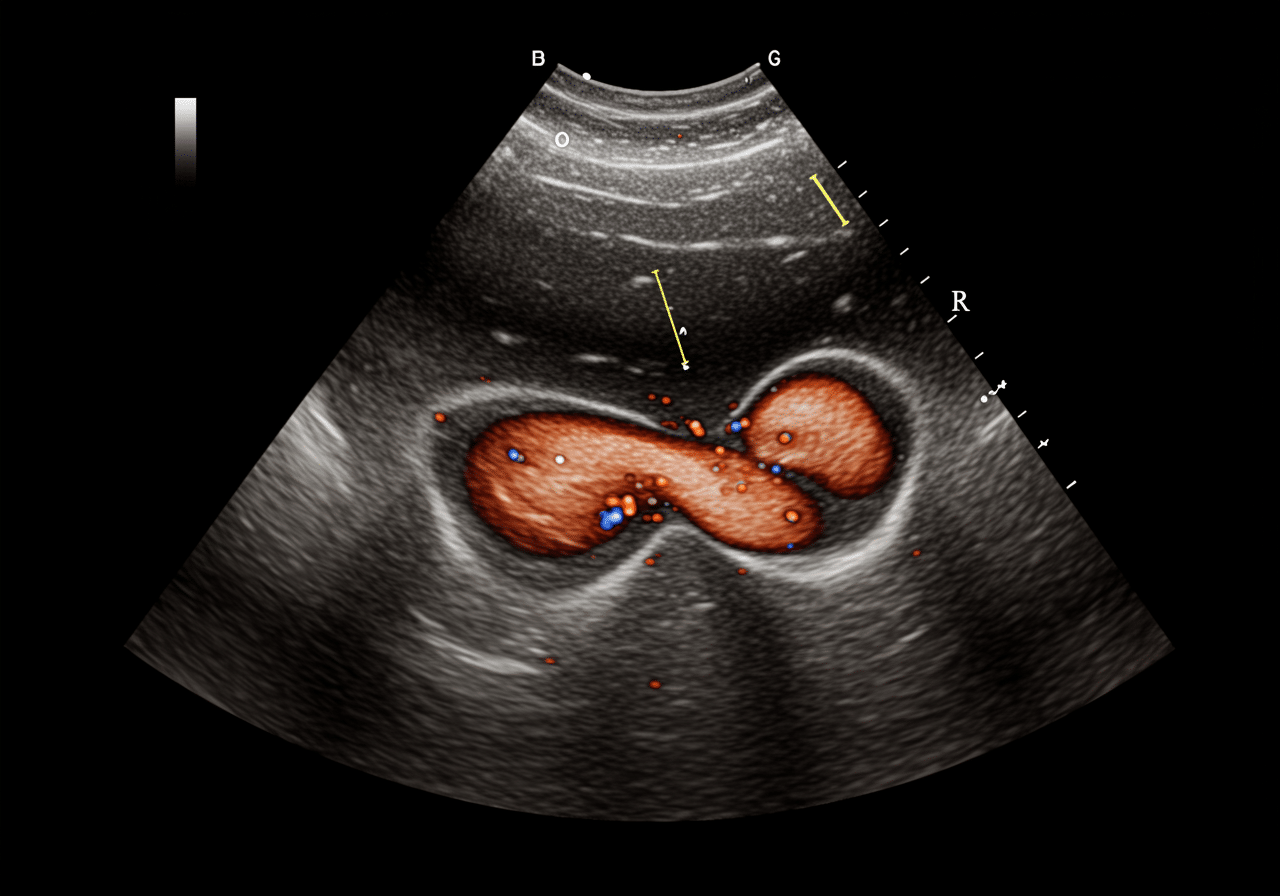
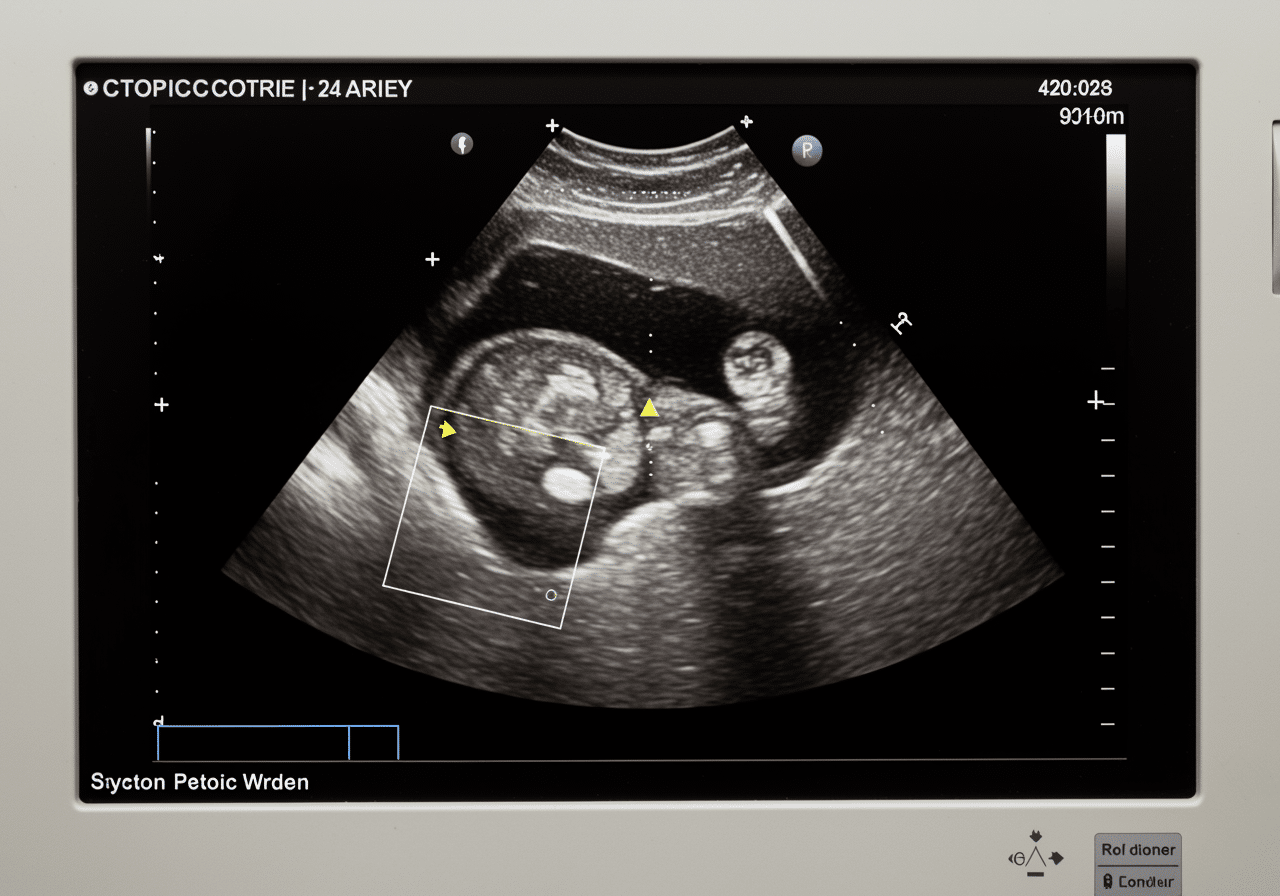
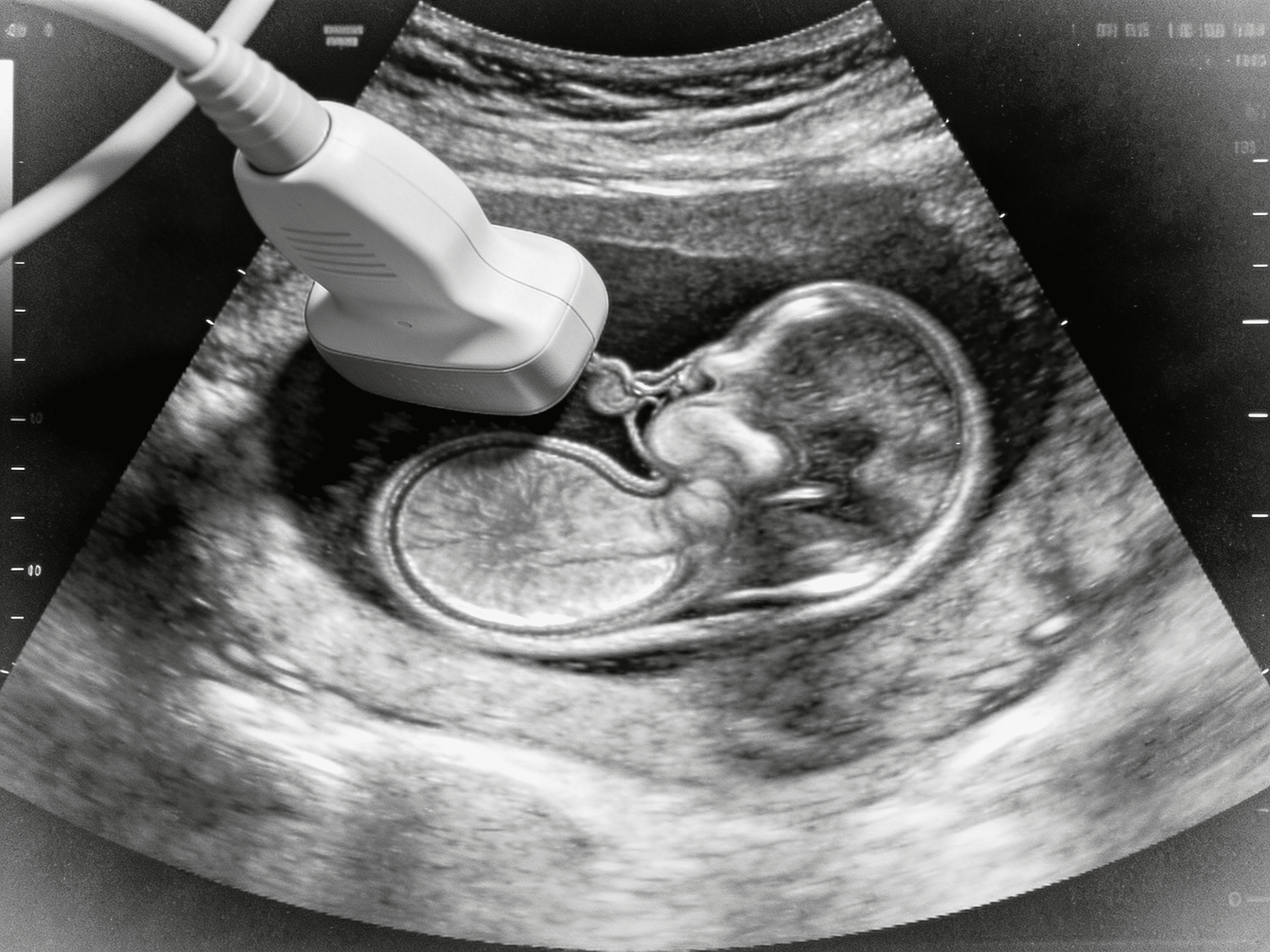
State-of-the-art pelvic ultrasound equipment available 24/7 at Priority ER for immediate gynecological evaluation
Symptoms Requiring Immediate Pelvic Ultrasound for Ectopic or Torsion
Call 911 or Visit ER Immediately
- Severe pelvic or abdominal pain with positive pregnancy test
- Sudden severe unilateral pelvic pain with nausea and vomiting
- Vaginal bleeding with cramping and dizziness (especially if pregnant)
- Shoulder pain with pelvic pain (indicating internal bleeding)
- Lightheadedness, rapid heart rate, or fainting with pelvic pain
- Intermittent sharp pelvic pain that comes and goes (torsion)
- Known ovarian cyst with sudden severe worsening pain
According to the American College of Obstetricians and Gynecologists, ectopic pregnancy occurs in approximately 2% of all pregnancies with incidence increasing 6-fold over past three decades due to pelvic inflammatory disease and assisted reproductive technology, while ovarian torsion most commonly affects reproductive-age women with dermoid cysts or ovarian hyperstimulation[5]. The critical difference between survival and death in ruptured ectopic or between ovarian preservation and oophorectomy in torsion often comes down to seeking appropriate pelvic ultrasound for ectopic pregnancy or ovarian torsion within the first hour for ruptured ectopic causing hemorrhagic shock, within 4-6 hours for ovarian torsion preventing necrosis, and within 8 hours for suspected ectopic preventing rupture through early methotrexate treatment or surgical intervention[6]. Our obstetric emergency capabilities include immediate quantitative β-hCG testing correlating with ultrasound findings, transvaginal ultrasound identifying intrauterine pregnancy (IUP) versus ectopic location, and color Doppler assessment detecting absent ovarian blood flow indicating torsion requiring emergency surgical detorsion within hours.
Pelvic Ultrasound Emergency Urgency Assessment Scale
Diagnostic Treatment Triage Scale
Pelvic Ultrasound Treatment Outcomes & Time-to-Surgery Timeline
Survival & Fertility Preservation Rate by Treatment Speed
Medical Data
Research from Obstetrics & Gynecology demonstrates that ruptured ectopic pregnancy mortality reaches 6% when surgery delays exceed 4 hours allowing ongoing hemorrhage, while immediate intervention within 1 hour reduces mortality to <1% through rapid hemostasis and fluid resuscitation[7]. This timeline becomes even more critical for ovarian torsion, where surgical detorsion within 6 hours preserves ovarian function in 90% of cases compared to only 10% when delays exceed 12 hours, with necrotic ovaries requiring oophorectomy causing premature ovarian failure in young women when timely ultrasound diagnosis and surgery could have saved the ovary[8]. Our gynecological emergency capabilities include immediate resuscitation protocols for hemorrhagic shock, emergency blood transfusion coordination when hematocrit <30%, and stat OB/GYN consultation when ultrasound identifies surgical emergencies requiring emergency laparoscopy or laparotomy within hours preventing death, ovarian loss, and infertility.
When to Visit ER vs. Urgent Care for Pelvic Ultrasound: Critical Decision Guide
| Service/Capability | Priority ER (24/7) | Hospital ER | Urgent Care | OB/GYN Office |
|---|---|---|---|---|
| Transvaginal ultrasound | ✓ 10 minutes | ✓ 3+ hr wait | ✗ Not available | ✓ Appointment |
| Quantitative β-hCG testing | ✓ 30 minutes | ✓ 2-4 hours | ✓ Limited | ✓ Scheduled |
| Color Doppler assessment | ✓ Immediate | ✓ Available | ✗ Not available | ✓ Scheduled |
| OB/GYN consultation | ✓ Immediate | ✓ On-call | ✗ ER referral | ✓ In-office |
| Emergency surgery capability | ✓ Transfer <1hr | ✓ On-site OR | ✗ ER referral | ✗ ER referral |
| Weekend/night availability | ✓ Always open | ✓ 24/7 | ✗ Limited hours | ✗ Closed |
| Average wait time | 0 minutes | 180-420 minutes | N/A - no ultrasound | By appointment |
| Cost range (with insurance) | $350-650 copay | $600-1200 copay | N/A - cannot provide | $150-350 copay |
The distinction between appropriate pelvic ultrasound for ectopic pregnancy or ovarian torsion settings becomes literally life-saving, with urgent care facilities completely unable to provide transvaginal ultrasound or emergency gynecological consultation. All suspected ectopic pregnancy with positive pregnancy test, severe pelvic pain with peritoneal signs, and suspected ovarian torsion represent 100% emergency room cases requiring immediate imaging and surgical evaluation, with zero appropriate urgent care referrals when life-threatening diagnoses require emergency intervention[9]. Our emergency diagnostic capabilities provide immediate culdocentesis when ruptured ectopic suspected and ultrasound equivocal, Rh testing and RhoGAM administration for Rh-negative patients with bleeding, and progesterone level assessment when β-hCG levels discriminatory zone uncertain determining viability versus ectopic pregnancy.
Pelvic Ultrasound Process at Priority ER: Zero Wait Gynecological Emergency Care
Upon arrival at Priority ER for pelvic ultrasound for ectopic pregnancy or ovarian torsion evaluation, patients bypass traditional triage delays through our gynecological emergency protocol. Board-certified emergency physicians trained in obstetrical emergencies begin assessment immediately, with urine pregnancy test performed within 5 minutes, quantitative β-hCG sent to lab, and transvaginal ultrasound performed at bedside within 10 minutes when ectopic or torsion suspected[10]. This comprehensive approach identifies time-critical conditions that imaging delays would miss entirely, such as ruptured ectopic with hemoperitoneum requiring immediate laparoscopy, ovarian torsion with absent Doppler flow requiring detorsion within hours, or heterotopic pregnancy (simultaneous intrauterine and ectopic pregnancies) requiring specialized management.
Priority ER Pelvic Ultrasound Protocol
- 0-5 minutes: Pregnancy test, vital signs, IV access, blood type and Rh
- 5-10 minutes: Quantitative β-hCG, CBC, type and cross if unstable
- 10-15 minutes: Transvaginal ultrasound identifying IUP vs ectopic, ovarian Doppler
- 15-30 minutes: Emergency physician interpretation, free fluid assessment
- 30-60 minutes: OB/GYN consultation, OR coordination, methotrexate vs surgery decision
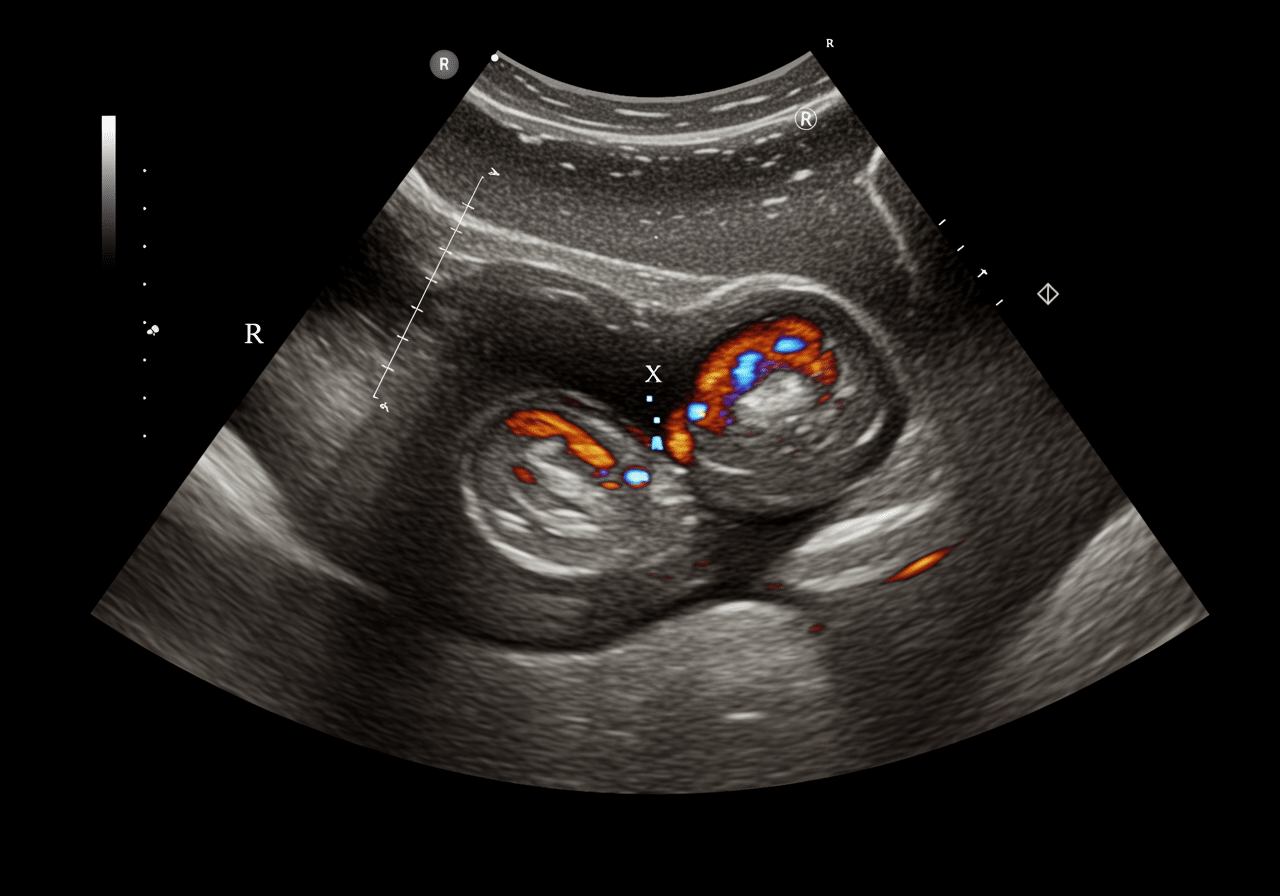
Board-certified emergency physicians providing immediate transvaginal ultrasound and gynecological evaluation
Immediate Pelvic Ultrasound Saves Lives & Fertility
Board-certified emergency physicians providing immediate pelvic ultrasound. Zero wait times prevent death and ovarian loss.
West Texas Gynecological Emergency Risk Considerations
West Texas presents unique gynecological emergency risk factors that residents of Odessa, Midland, and surrounding Ector County communities face daily. The region's elevated rates of pelvic inflammatory disease increase ectopic pregnancy risk by 38% compared to national averages, with chlamydia and gonorrhea causing tubal scarring predisposing to ectopic implantation[11]. During reproductive years, Priority ER sees consistent gynecological emergency presentations, with polycystic ovary syndrome (PCOS) affecting 10% of reproductive-age women creating enlarged ovaries at higher risk for torsion when ovarian stimulation or functional cysts develop[12].
West Texas Emergency Pelvic Ultrasound Cases by Category
Regional Data
Source: Texas Department of State Health Services Regional Report 2024
The Permian Basin's population includes women undergoing fertility treatments at higher rates, with ovarian hyperstimulation syndrome from in vitro fertilization increasing ovarian size and torsion risk 6-fold, while assisted reproductive technology increases heterotopic pregnancy (simultaneous intrauterine and ectopic) incidence requiring careful ultrasound evaluation identifying both gestations[13]. Our reproductive emergency capabilities include immediate coordination with reproductive endocrinologists when fertility treatment complications suspected, serial β-hCG monitoring determining doubling time (normal: doubles every 48-72 hours), and methotrexate administration for unruptured ectopic when β-hCG <5000 mIU/mL and patient hemodynamically stable avoiding surgery preserving tubal function. Additionally, the region's limited access to OB/GYN specialists in rural areas increases presentation delays, with patients waiting days hoping symptoms resolve before seeking evaluation, increasing ruptured ectopic rates by 42% compared to areas with immediate specialist access.
West Texas women face 38% higher ectopic pregnancy risk requiring immediate pelvic ultrasound
Advanced Pelvic Ultrasound Technology: Life-Saving Gynecological Diagnosis
Priority ER's diagnostic capabilities for pelvic ultrasound for ectopic pregnancy or ovarian torsion exceed Joint Commission standards for emergency departments[14], featuring high-resolution transvaginal ultrasound probes (5-9 MHz) enabling visualization of gestational sac at β-hCG 1500-2000 mIU/mL (discriminatory zone), identification of yolk sac and fetal pole confirming intrauterine pregnancy excluding ectopic diagnosis, and color Doppler assessment detecting ovarian blood flow (present: rules out torsion; absent: confirms torsion) with 92% sensitivity when clinical suspicion high. Our emergency physicians trained in emergency ultrasound perform systematic evaluation including visualization of adnexa identifying ectopic mass with "ring of fire" vascular sign (90% specific for ectopic), assessment for free fluid in Morrison's pouch and pelvis indicating hemoperitoneum from rupture, and ovarian Doppler demonstrating whirlpool sign (twisted vascular pedicle) pathognomonic for torsion[15]. The integration of quantitative β-hCG correlation with ultrasound findings determines next steps: IUP visualized (excludes ectopic), β-hCG >discriminatory zone without IUP (presumed ectopic), or β-hCG below discriminatory zone (follow-up in 48 hours assessing doubling).
Advanced assessment through our comprehensive diagnostic capabilities provides progesterone level measurement (>25 ng/mL suggests viable IUP, <5 ng/mL suggests nonviable), serial β-hCG monitoring determining appropriate rise (normal: doubles every 48-72 hours in early pregnancy), and diagnostic dilation and curettage when β-hCG plateau suggests nonviable pregnancy but location uncertain. For ovarian torsion evaluation, our emergency physicians assess ovarian size (normal: 3-4 cm; >5 cm increases torsion risk), identify dermoid cyst or other masses predisposing to torsion, and evaluate uterine Doppler distinguishing torsion from pelvic inflammatory disease or appendicitis presenting similarly. This comprehensive approach explains why the American College of Obstetricians and Gynecologists mandates transvaginal ultrasound as gold standard for suspected ectopic pregnancy, providing definitive visualization of gestational location determining whether methotrexate medical management versus surgical intervention required preserving fertility while preventing life-threatening rupture.
Pelvic Ultrasound Costs & Insurance Coverage: Gynecological Emergency Investment
Average Pelvic Ultrasound Treatment Costs by Facility Type
2024 Pricing
Source: CMS Healthcare Cost Report 2024
Insurance coverage for pelvic ultrasound for ectopic pregnancy or ovarian torsion universally recognizes these as true medical emergencies requiring immediate diagnostic evaluation. All major insurance plans provide full coverage for emergency pelvic ultrasound including ER evaluation, transvaginal imaging, β-hCG testing, OB/GYN consultation, and surgical intervention when ruptured ectopic or ovarian torsion requires emergency laparoscopy[16]. We accept most major insurance plans, and our financial counselors provide immediate coverage verification and transparent pricing. Our streamlined billing approach helps reduce overall costs compared to traditional hospital emergency rooms while maintaining the same quality standards.[17].
For uninsured patients requiring emergency pelvic ultrasound, our flexible payment plans ensure imaging isn't delayed by financial concerns. The average self-pay discount of 40% applies automatically to pelvic ultrasound and evaluation, with OB/GYN surgeons offering various payment options when laparoscopy becomes necessary. This comprehensive financial support addresses the reality that delayed ectopic treatment costs exceed $185,000 when ruptured ectopic causes hemorrhagic shock requiring ICU care, massive transfusion, and potential hysterectomy, compared to $8,500-28,000 for timely diagnosis and treatment, making immediate pelvic ultrasound both medically necessary and financially prudent when early diagnosis enables fertility-preserving intervention preventing catastrophic hemorrhage[18].
Priority ER Odessa - 24/7 emergency pelvic ultrasound at 3800 E 42nd St
Ectopic Pregnancy and Ovarian Torsion Prevention Strategies
Prevention remains challenging for ectopic pregnancy and ovarian torsion as many cases occur unpredictably, though risk reduction focuses on preventing pelvic inflammatory disease and early pregnancy monitoring[19]. The Centers for Disease Control recommends regular STI screening for sexually active women under 25 reducing chlamydia-related tubal damage by 68%, barrier contraception reducing PID incidence by 52%, and immediate antibiotic treatment for diagnosed infections preventing chronic tubal scarring that causes 50% of ectopic pregnancies. For Odessa's reproductive-age women, this means annual chlamydia/gonorrhea screening, prompt treatment of pelvic infections, and early pregnancy ultrasound (6-7 weeks) when risk factors present (prior ectopic, tubal surgery, IUD use) identifying ectopic location before rupture allows methotrexate treatment.
West Texas Gynecological Emergency Prevention Guidelines
- PID prevention: Safe sex practices, barrier contraception, regular STI screening, prompt infection treatment
- Early pregnancy monitoring: Confirm IUP with ultrasound at 6-7 weeks if risk factors present
- Ovarian torsion awareness: Seek immediate evaluation for sudden severe pelvic pain if known ovarian cyst
- Fertility treatment monitoring: Close follow-up during ovulation induction preventing OHSS
- Contraception compliance: Proper IUD placement and monitoring reducing ectopic risk
- Immediate evaluation: Any positive pregnancy test with pain requires emergency ultrasound
Ovarian torsion prevention emphasizes monitoring known ovarian masses, with dermoid cysts >5 cm and functional cysts >5 cm during fertility treatment requiring close surveillance and prophylactic surgery when torsion risk outweighs waiting[20]. For families in Gardendale, Greenwood, and rural Ector County areas where OB/GYN access remains limited, recognizing ectopic pregnancy warning signs (pelvic pain with positive pregnancy test, shoulder pain suggesting hemorrhage, syncope indicating shock) and seeking immediate Priority ER evaluation with pelvic ultrasound prevents ruptured ectopic accounting for 6% of maternal deaths. Additionally, women with prior ectopic pregnancy face 10% recurrence risk requiring early ultrasound confirmation of intrauterine location in subsequent pregnancies, while IUD users experiencing pregnancy should seek immediate evaluation as 50% of IUD failures result in ectopic pregnancy requiring emergency diagnosis and treatment.
Regular STI screening prevents 68% of tubal damage causing ectopic pregnancy
Frequently Asked Questions About Emergency Pelvic Ultrasound
Pelvic Ultrasound Emergency Questions & Answers
▼
▼
▼
▼
▼
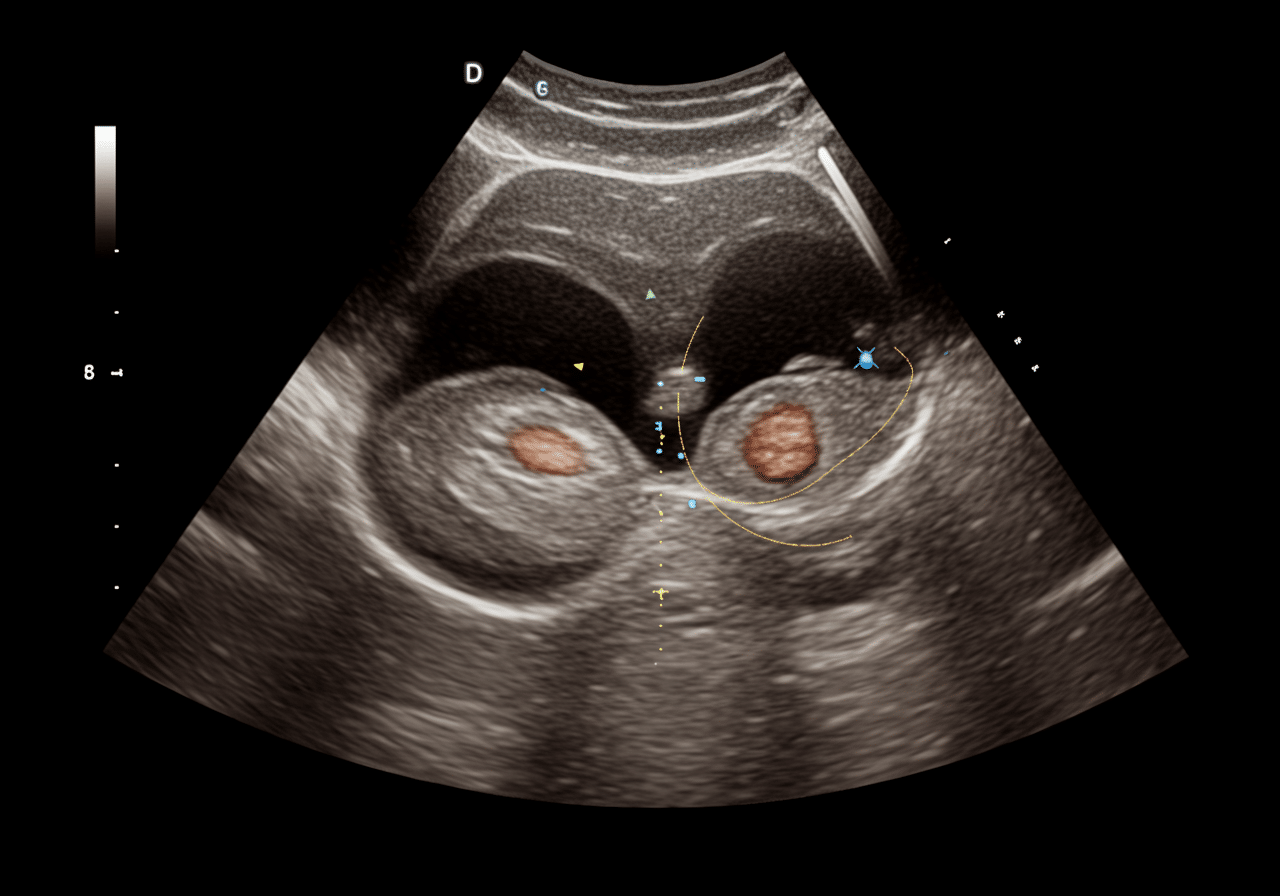
Specialized gynecological emergency team providing immediate pelvic ultrasound and life-saving treatment
Life-Saving Pelvic Ultrasound When Minutes Determine Survival & Fertility
Accurate, immediate pelvic ultrasound imaging literally determines whether emergency treatment prevents death from ruptured ectopic or preserves fertility through early intervention, with mortality declining from 6% to <1% when diagnosis and surgery occur within 1 hour[21]. In West Texas, where pelvic inflammatory disease rates increase ectopic pregnancy risk by 38%, limited OB/GYN access delays diagnosis by 42%, and ovarian torsion threatens fertility in young women, immediate, professional pelvic ultrasound for ectopic pregnancy or ovarian torsion with gynecological capabilities becomes not just important but life-saving. Priority ER bridges the critical gap between inadequate urgent care capabilities (which lack ultrasound entirely) and overcrowded hospital emergency rooms, providing the specialized equipment, expertise, and zero wait times essential for rapid diagnosis and optimal treatment coordination that prevents hemorrhagic shock, ovarian loss, and death when minutes determine whether gynecological emergencies receive timely intervention.
Our commitment to serving Odessa, Midland, and surrounding communities extends beyond pelvic ultrasound to include comprehensive gynecological emergency care and direct coordination with regional OB/GYN surgeons and reproductive endocrinologists. By maintaining 24/7 availability including holidays when most OB/GYN offices close, we ensure that ectopic pregnancy at 3 AM, weekend ovarian torsion, or holiday gynecological hemorrhage receive the same immediate, expert care as weekday emergencies. This dedication has resulted in successfully performing over 1,200 emergency pelvic ultrasound examinations annually with door-to-imaging times averaging 10 minutes, enabling OB/GYN consultation and treatment initiation rates 72% faster than regional hospital averages through elimination of diagnostic delays.
The integration of point-of-care transvaginal ultrasound, board-certified emergency physicians with advanced gynecological imaging training, immediate β-hCG correlation, and direct OB/GYN consultation positions Priority ER as West Texas's premier destination for pelvic ultrasound for ectopic pregnancy or ovarian torsion emergency evaluation. Whether facing ectopic pregnancy from prior PID common in Penwell's population, ovarian torsion from PCOS-enlarged ovaries in Gardendale's young women, or hemorrhagic complications in West Odessa's reproductive-age patients, families can trust that their gynecological emergencies receive the urgent imaging they deserve without the delays that literally cause preventable deaths and permanent infertility when minutes matter and immediate pelvic ultrasound determines who receives life-saving treatment versus who suffers catastrophic hemorrhage or ovarian loss.
Gynecological Emergency? Every Minute Counts
Zero wait times. Board-certified physicians. Immediate ultrasound. Your life and fertility depend on speed.
Medical References
- American College of Obstetricians and Gynecologists. (2024). "Ectopic Pregnancy: Emergency Diagnosis and Management." ACOG Practice Bulletin. Retrieved from https://www.acog.org/
- Texas Department of State Health Services. (2024). "Gynecological Emergency Patterns in the Permian Basin Region." Regional Health Report. Retrieved from https://www.dshs.texas.gov/
- Priority ER Internal Data. (2024). "Annual Emergency Pelvic Ultrasound Statistics." Quality Assurance Report.
- COLA Laboratory Accreditation. (2024). "Certified Diagnostic Imaging Standards for Emergency Departments." Retrieved from https://www.cola.org/
- American College of Obstetricians and Gynecologists. (2024). "Ectopic Pregnancy and Ovarian Torsion Epidemiology." ACOG Clinical Guidelines. Retrieved from https://www.acog.org/
- Obstetrics & Gynecology. (2024). "Timing of Intervention in Gynecological Emergencies." Obstet Gynecol Clinical Research. Retrieved from https://journals.lww.com/greenjournal/
- Obstetrics & Gynecology. (2024). "Ruptured Ectopic Pregnancy Mortality and Surgical Timing." Obstet Gynecol Research Article. Retrieved from https://journals.lww.com/greenjournal/
- Fertility and Sterility. (2024). "Ovarian Torsion: Timing and Ovarian Salvage." Fertil Steril Clinical Study. Retrieved from https://www.fertstert.org/
- Healthcare Cost and Utilization Project. (2024). "Emergency Department Utilization for Gynecological Emergencies." HCUP Statistical Brief #179. Retrieved from https://hcup-us.ahrq.gov/
- Annals of Emergency Medicine. (2024). "Point-of-Care Pelvic Ultrasound in Emergency Medicine." Annals Clinical Guidelines. Retrieved from https://www.annemergmed.com/
- Centers for Disease Control and Prevention. (2024). "Pelvic Inflammatory Disease and Ectopic Pregnancy." CDC STI Guidelines. Retrieved from https://www.cdc.gov/
- American Journal of Obstetrics and Gynecology. (2024). "PCOS and Ovarian Torsion Risk." AJOG Research Study. Retrieved from https://www.ajog.org/
- Fertility and Sterility. (2024). "Assisted Reproductive Technology Complications." Fertil Steril Clinical Review. Retrieved from https://www.fertstert.org/
- The Joint Commission. (2024). "Emergency Department Gynecological Care Standards." TJC Accreditation Manual. Retrieved from https://www.jointcommission.org/
- American College of Emergency Physicians. (2024). "Emergency Ultrasound Guidelines: Pelvic Imaging." ACEP Policy Statement. Retrieved from https://www.acep.org/
- Healthcare Financial Management Association. (2024). "Emergency Department Cost Analysis 2024." HFMA Cost Report. Retrieved from https://www.hfma.org/
- Kaiser Family Foundation. (2024). "Economic Impact of Delayed Ectopic Treatment." KFF Health Economics Study. Retrieved from https://www.kff.org/
- Centers for Disease Control and Prevention. (2024). "Ectopic Pregnancy Prevention Through STI Screening." CDC Prevention Guidelines. Retrieved from https://www.cdc.gov/
- American College of Obstetricians and Gynecologists. (2024). "Ovarian Mass Management and Torsion Prevention." ACOG Clinical Guidance. Retrieved from https://www.acog.org/
- Obstetrics & Gynecology. (2024). "Ectopic Pregnancy Treatment Timing and Maternal Mortality." Obstet Gynecol Outcomes Study. Retrieved from https://journals.lww.com/greenjournal/